
Kathy Schneider, PhD, Miriam Isola, DrPH CPHIMS, and David Troiano, RPh, MSIA, CPPS
Background
The opioid epidemic in the US is widely recognized as a health crisis. Opioids are drugs used to manage severe pain. According to a report published by the CDC over 50 million people in the US suffer from chronic or persistent pain[1] ; many more experience acute pain. Control of pain is one of the main reasons people seek medical care and is the starting point for the national problem of opioid dependence. Chronic pain contributes to the high cost of healthcare, lost productivity and disability[2].
According to the US Drug Enforcement Administration (DEA), commonly used drugs include prescription medications such as oxycodone, hydrocodone, fentanyl, oxymorphone, and methadone which are Schedule II drugs under the Controlled Substances Act (CSA); heroin, which is not available by prescription, also falls into this category[3]. Regular use, even as prescribed by a doctor, can cause serious harm, including dependence, overdose and death.
The use of opioids in the US has increased dramatically over the past two decades. The volume of opioids prescribed in 2015 was approximately three times higher than in 1999[4]. The Centers for Disease Control and Prevention (CDC) reported that from 2000 to 2014, the rate of deaths from drug overdoses increased 137%, including a 200% increase in the rate of overdose deaths involving opioids (e.g., opioid pain relievers and heroin)[5]. Even with the growing attention to this public health crisis, the US continues to see a rise in opioid deaths. In 2017 67.8% of overdose deaths were due to opioids [6].
Inpatient hospital stays related to opioid overuse increased from 116.7 per 100,000 in 1992 to 295.6 per 100,000 in 2012[7]. Rates of emergency department (ED) utilization due to opioid use or misuse doubled from 2005 – 2014 from 89.1 to 177.7 visits per 100,000 patients[8], and rates continued to climb to 241 visits per 100,000 in 2016 – the most recently reported data[9]. Between 24 and 27 percent of drug-related ED visits become hospital admissions, which further increases the cost of care[10].
Many new opioid pain medicines have been approved by the Federal Drug Administration (FDA) over the last 20 years, including formulations designed to be long-acting (controlled-release) such as oxycontin, or easier to use (transdermal patches or transmucosal lollipops [Actiq]) such as fentanyl[11]. More people are exposed to prescription opioids than ever before. Opioids can cause side effects and adverse events even when used as prescribed; furthermore, the risk of addiction is forever present – with some populations being particularly vulnerable to dependence. Additional problems arise when opiates are not prescribed in accordance with clinical guidelines; recently guidelines have been tightening up recommendations for screening patients before prescribing opioids – and limiting the morphine milligram equivalents (MME) and duration (i.e., days supply of the medication and avoiding long-acting forms) of opiate prescriptions.
Federal, state and local health authorities are eager for solutions to reduce patient harm and mortality related to opioid use. In 2015 the U.S. HHS has issued a 5-point strategy to address the opioid issue[12], with the key priority to improve opioid prescribing practices.
Understanding Patient Needs for pain management
Over the last few decades, many providers have approached the need for pain control by increased prescribing of opiates and have shifted away from the many non-opiate (e.g. ibuprofen) and nonpharmacologic (e.g. heat, acupuncture, physical therapy, exercise) alternatives. A plethora of clinical practice guidelines recommend practices for specific populations (e.g., surgical pain[13], back pain[14], chronic pain[15]). To meet patient needs for pain management and at the same time avoid over-prescribing, providers must consider personalized approaches to diagnosis and treatment of pain.
A methodical approach to examining pain management and prescribing practices will identify demographic groups and special populations, such as older adults, individuals with co-morbidities, and cognitive impairment that often require pain management and alternatives to opioids. If this information is provided to an interdisciplinary team that includes prescribers, pharmacists and epidemiologists it will lead to a comprehensive solution that considers perspectives that are not only medical, but also population-based and incorporate expertise from pharmacy.
Examining Prescriber Practices
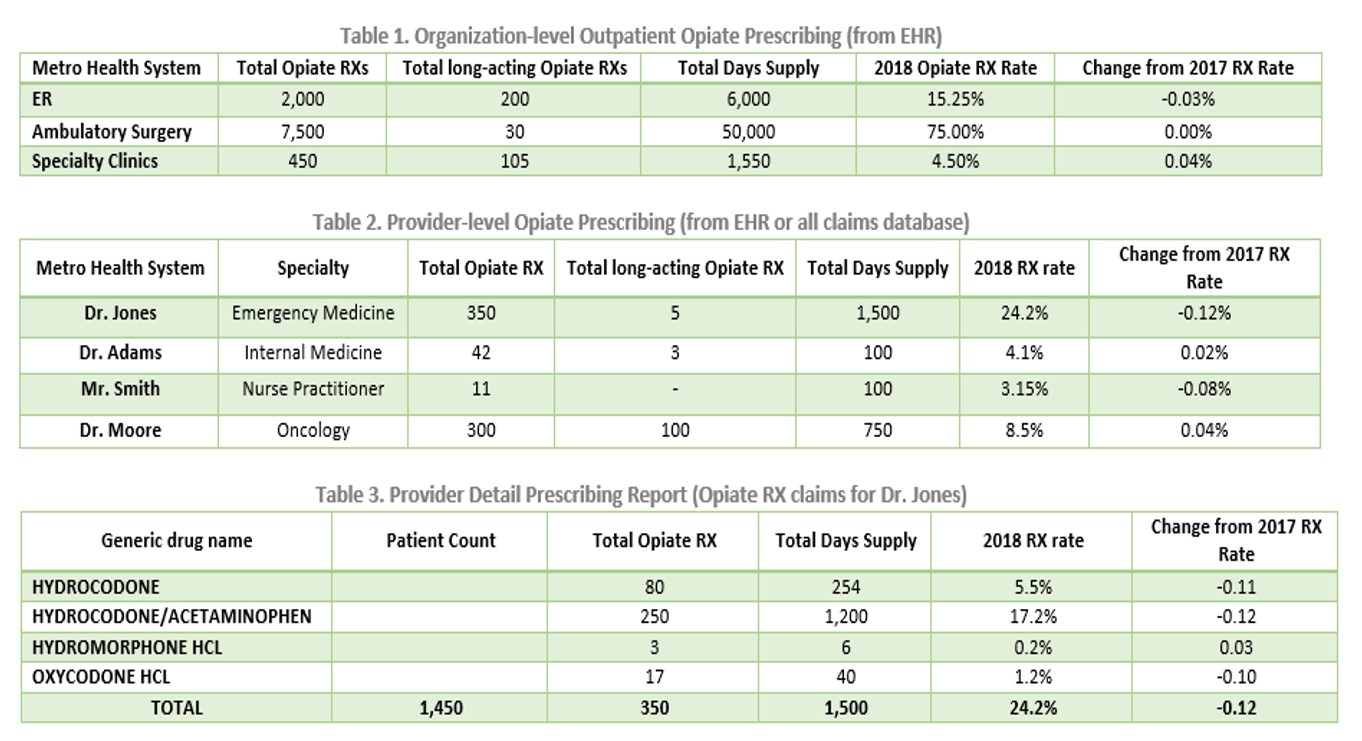
A data-driven approach examining organizational and provider-level prescribing practices is essential to identify areas for improvement. Using clinical practice guidelines and best practices in pain control – we compare actual opioid prescribing practices to the desired/recommended patterns. Organizations can leverage their prescribing data from the EHR to analyze the data by organization or department, by provider and by medication such as in Tables 1 – 3.
Furthermore, providers benefit from detailed information regarding their patient population. Examining patient risk profiles along with prescribing data highlights areas where improved prescribing practices and pain management strategies are needed. Table 4 is an example of risk factors providers may wish to monitor. A list of patients with particular risk factors can also be obtained.

Improving Prescriber Practices
One of the most productive places to reduce the risk of harm through opioid use and misuse is through improved prescribing of these beneficial but potentially harmful medications. A nuanced approach to examining prescribing data is needed. Depicting overall opiate prescription rates is not sufficient for improving prescriber practices; as we demonstrate, drilling down further into the data is essential. Beyond examining data, collaborative decision-making with patients is needed – where providers communicate with patients about their pain control needs.
Providers should avoid prescribing narcotic pain relievers whenever possible – and even then, the lowest dosage for the shortest duration possible is prudent[16]. Furthermore, there are patients for whom opiates should not be dispensed as the first choice for managing pain; this includes patients who are at high risk for addiction. There are many different types of pain control options, including multidisciplinary and multimodal efforts that include rehabilitation therapy, and non-opioid analgesics. A broad perspective on approaches to pain control should be adopted[17].
Another subgroup of patients in need of careful monitoring for appropriateness of ongoing medication use are those who are already receiving opiates and are requesting a refill. For patients requesting refills of opiate prescriptions, this may be an opportune time to cease or taper the dosage. A stated treatment goal should be to avoid dependence on opiates[18] and avoid switching to other habit-forming drugs.Yet another subgroup of patients includes those who have chronic pain, for whom other therapies have failed. Carefully tailored treatment plans are in order to address patient needs for chronic pain relief. There are clinical practice guidelines for pain control in chronic pain non-cancer patients [19]. Although some chronic pain patients may already be managed using long-term opioid therapy (LTOT), it is important for providers to work with patients so that there is not an expectation that they will be pain-free; staying within a tolerable threshold of pain should be the therapeutic goal. For LTOT patients, it’s particularly important to take an interdisciplinary approach – with careful monitoring to be sure clinical guidelines are being followed.
Patient Engagement around the issue of pain management and opiate avoidance can be challenging, particularly if patients have experienced benefits from the medication. A primary goal of improving provider practices should be to avoid having appropriate pain management develop into drug dependence. Providers must engage in conversations with their patients about what non-narcotic solutions will be acceptable to manage pain[20]. Ideally, prescribers should work with pharmacists on the care team to carefully monitor opiate prescriptions. Pharmacists contribute much expertise which can help in forming an acceptable pharmacologic solution; this may be an iterative process of adjusting dosages and formulations until an appropriate pain control solution is reached.
In addition to using your in-house EHR data, some states have established prescription drug monitoring programs (PDMPs)[21], and have databases that could be used to examine prescriber opioid practices. This is an improvement on traditional utilization management approaches. Accessing information from a clearinghouse (other examples may include health information exchanges [HIEs], pharmacy insurance claims, etc.) will allow a broader view of prescriber and patient activity and can be useful to help providers make the most informed choice for what is best for the patient.
Conclusions
Sum-IT Health Analytics provides custom analytic solutions to align with your patient care methodologies and clinical workflows. These solutions leverage your prescribing data and turn it into actionable information that can be used to improve prescriber practices. We compare observed prescribing to the relevant clinical practice guidelines to identify areas for intervention. Some prescribers may have high proportions of patients for whom they prescribe opiates; furthermore, some providers may prescribe long duration or high dosages of MME for their patients (e.g., fentanyl). All of these prescribing practices should be examined to reduce the risk of harm to patients.
Health organizations need actionable data: which providers, which patients, which medications may require modification? Making this information available to providers is an effective tool for improving prescriber practices[22]. We need to assist providers to employ alternative (non-narcotic) pain management strategies ensure that patients are using addictive drugs for only very short time frames. There is an inherent need for providers to work with patients to achieve pain control, however we must work toward non-narcotic options.
Contact us to learn more about how we can collaborate with your organization to improve prescribing practices.
Contact Sum-IT or the authors at:
Miriam Isola, DrPH, CPHIMS Kathy Schneider, PhD
847-975-2141 515-771-3981
Co-Founder and Chief Strategy Officer Co-Founder and Epidemiologist
Miriam.Isola@sumithealthanalytics.com Kathy.Schneider@sumithealthanalytics.com
http://www.sumithealthanalytics.com/
[1] Dahlhamer J, Lucas J, Zelaya, C, et al. Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults — United States, 2016. MMWR Morb Mortal Wkly Rep 2018;67:1001–1006. DOI: http://dx.doi.org/10.15585/mmwr.mm6736a2external icon.
[2] Institute of Medicine. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. Washington, DC: National Academies Press; 2011. https://www.nap.edu/read/13172/chapter/1
[3] U.S. Drug Enforcement Administration, Office of Diversion Control. (2015). National Forensic Laboratory Information System Special Report: Opiates and Related Drugs Reported in NFLIS, 2009–2014. Springfield, VA: U.S. Drug Enforcement Administration. https://www.deadiversion.usdoj.gov/nflis/spec_rpt_opioids_2014.pdf
[4] Guy GP Jr., Zhang K, Bohm MK, et al. Vital Signs: Changes in Opioid Prescribing in the United States, 2006–2015. MMWR Morb Mortal Wkly Rep 2017;66:697–704. DOI: http://dx.doi.org/10.15585/mmwr.mm6626a4
[5] Increases in Drug and Opioid Overdose Deaths — United States, 2000–2014. January 1, 2016 / 64(50);1378-82. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6450a3.htm
[6] Scholl L, Seth P, Kariisa M, Wilson N, Baldwin G. Drug and Opioid-Involved Overdose Deaths — United States, 2013–2017. MMWR Morb Mortal Wkly Rep 2019;67:1419–1427. DOI: http://dx.doi.org/10.15585/mmwr.mm675152e1
[7] Owens PL, Barrett ML, Weiss AJ, Washington RE, Kronick R. Hospital Inpatient Utilization Related to Opioid Overuse Among Adults, 1993-2012. HCUP Statistical Brief #177. August 2014. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb177-Hospitalizations-for-Opioid-Overuse.pdf.
[8] Weiss AJ, Bailey MK, O’Malley L, Barrett ML, Elixhauser A, Steiner CA. Patient Characteristics of Opioid-Related Inpatient Stays and Emergency Department Visits Nationally and by State, 2014. HCUP Statistical Brief #224. June 2017. Agency for Healthcare Research and Quality, Rockville, MD. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb224-Patient-Characteristics-Opioid-Hospital-Stays-ED-Visits-by-State.pdf
[9] HCUP Fast Stats. Healthcare Cost and Utilization Project (HCUP). April 2019. Agency for Healthcare Research and Quality, Rockville, MDhttps://www.hcup-us.ahrq.gov/faststats/OpioidUseServlet?radio-3=on&location1=US&characteristic1=01&setting1=ED&location2=&characteristic2=01&setting2=IP&expansionInfoState=hide&dataTablesState=hide&definitionsState=hide&exportState=hide Accessed 7/27/2019.
[10] Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. The DAWN Report: Highlights of the 2011 Drug Abuse Warning Network (DAWN) Findings on Drug-Related Emergency Department Visits. Rockville, MD. https://www.samhsa.gov/data/sites/default/files/DAWN127/DAWN127/sr127-DAWN-highlights.htm
[11] Food and Drug Administration. “Timeline of Selected FDA Activities and Significant Events Addressing Opioid Misuse and Abuse.” https://www.fda.gov/drugs/information-drug-class/timeline-selected-fda-activities-and-significant-events-addressing-opioid-misuse-and-abuse . Downloaded 7/4/2019.
[12] US HHC “Opioids: The Prescription Drug & Heroin Overdose Epidemic.” Webpage. https://www.hhs.gov/opioids/
[13] Bree Collaborative. “Prescribing Opioids for Postoperative Pain – Supplemental Guide.” July 2018. http://www.agencymeddirectors.wa.gov/Files/FinalSupBreeAMDGPostopPain091318wcover.pdf
[14] Qaseem A, Wilt TJ, McLean RM and Forciea MA. “Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians.” Ann Int Med. 2017;166(7):514-530. DOI: 10.7326/M16-2367
[15] Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016. MMWR Recomm Rep 2016;65(No. RR-1):1–49. DOI: http://dx.doi.org/10.15585/mmwr.rr6501e1external icon.
[16] Pino CA and Covington M. “Prescription of opioids for acute pain in opiate naïve patients.” UpToDate. May 14, 2019. https://www.uptodate.com/contents/prescription-of-opioids-for-acute-pain-in-opioid-naive-patients. Accessed 7/18/2019.
[17] Kroenke K, Alford DP, Argoff C, Canlas B, Covington E et al. “Challenges with Implementing the Centers for Disease Control and Prevention Opioid Guideline: A Consensus Panel Report.” Pain Medicine 2019; 20(4): 724-735. doi: 10.1093/pm/pny307
[18] American Psychiatric Association. Opioid Use Disorder. https://www.psychiatry.org/patients-families/addiction/opioid-use-disorder/opioid-use-disorder. Accessed 7/19/2019.
[19] Califf RM, Woodcock J and Ostroff S. “Special Report: A Proactive Response to Prescription Opioid Abuse.” NEJM, April 14, 2016; 374(15): 1480- 1485.
[20] Kroenke K, et al. op. cit.
[21] Centers for Disease Control and Prevention. What States Need to Know about PDMPs. https://www.cdc.gov/drugoverdose/pdmp/states.html . Accessed 7/27/2019.
[22] Partnership for Health IT Patient Safety. Safe Practice Recommendations for Safer Opioid Prescribing: Measures and Clinical Decision Support. White paper. ECRI Institute& HIMSS, 2019. https://assets.ecri.org/PDF/HIT-Partnership/EHRA-ECRI-Safe-Opioid-White-Paper-Final.pdf